Is it good or bad when the placenta is located on the back wall of the uterus? Pregnancy and location of the placenta.
Types of abnormal location of the placenta (Fig. 55, a, b, c). If the placenta, at least in some part, is located closer than 7 cm from the internal os, this means that it is partially attached (primarily or secondary) to that part of the uterus that stretches during childbirth, since the final deployment of the lower part of the uterus occurs in this part of the uterus. segment. This location of the placenta is called low location.
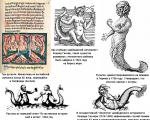
Rice. 55. Main types of placenta previa. a - marginal; b - lateral; in - central.
If the placenta, located in the lower segment, reaches the edge of the internal os, they speak of marginal presentation (placenta praevia marginalis). Thus, the low location of the placenta is a transitional stage between its normal location and lateral presentation.
When the internal os is partially blocked by the placenta, they speak of lateral (or partial) placenta previa (placenta praevia lateralis seu paritalis).
If the internal pharynx is completely blocked by the placenta, they speak of complete presentation (placenta praevia totalis s. centralis), regardless of whether the pharynx corresponds to the center of the placenta or not.
Some authors allow differentiation of typical forms of placenta previa with full opening of the pharynx, others - only with some opening of it, and still others (as is customary in our clinic) - with any opening, if only placental tissue is found everywhere in the area of the internal pharynx. In the latter case, they speak of complete placenta previa. This definition does not contradict the fact that with a larger opening, for example three fingers, only the edge of the placenta can be detected and it is quite advisable, since treatment for placenta praevia should begin even before the cervix is completely opened.
However, it should be noted that the latter classification is scientifically inaccurate, and is convenient only from a practical point of view. In this regard, we fully agree with G. G. Genter, who believed that it is necessary to distinguish whether, with sufficient opening, only the tissue of the placenta or its tissue together with the membranes is determined. It is clear that with the onset of labor and with the expansion of the internal os, placenta praevia marginalis can turn into placenta praevia lateralis, and placenta praevia centralis - placenta praevia lateralis.
Measuring the distance from the site of rupture of the membranes to the edge of the born placenta is of interest in that it allows one to check the type of placenta previa. So, with a low location of the placenta, the rupture of the membranes is 3-4 cm from its edge; with placenta praevia marginalis, it is located along its edge, while with the normal location of the placenta, the place of the rupture is 7-10 cm or more from the edge of the placenta.
If the placenta develops in the cervical canal, then they speak of cervical placenta previa (placenta cervicalis).
However, it should be borne in mind that in some cases there may not be clear boundaries of the location of the placenta, corresponding to the topographic boundaries of the uterus, and so-called transitional forms occur.
This means that some part of the placenta (its individual lobules) can pass either from the cervical canal (in the presence of a cervical pregnancy) to the region of the lower segment, or, conversely, from the lower segment to the wall of the cervix, growing in individual lobules into the latter or hanging down (in in the form of a small flap) into the lumen of the cervical canal.
In accordance with everything said above, we can assume that the classification of the possible location of the placenta proposed by V. M. Malyavinsky is completely justified in scientific and practical terms. He distinguishes three types of location of the placenta in the uterine cavity (Fig. 56): 1) within the boundaries of the uterine body (placenta corporalis), 2) completely or partially in the area of the isthmus (placenta isthmica) and 3) in the cervical canal (placenta cervicalis). Of these three types of placenta location, only the last two are previa. Therefore, with the introduction of V. M. Malyavinsky’s terminology into use, the term “presentation” (praevia) becomes completely unnecessary.
Each of the listed types of placenta location has several variations.
Placenta praevia occurs on average once per 500-600 births, or in 0.17% (M. V. Florov). According to V. M. Mikhailov, the frequency of placenta praevia is 1: 276, according to N. I. Pobedinsky - 1: 250. A. A. Ivanova - 1: 266, E. B. Derankova - 1: 179. This difference in the frequency of placenta previa is explained by the fact that the authors do not adhere to a single classification.

Rice. 56. Types of placenta location according to Malyavinsky.
a - placenta corporalis; b - pl. isthmica; in - pl. cervicalis; 1 - body of the uterus; 2 - isthmus; 3 - neck.
In general, a low location of the placenta occurs in 60-70% of all births with placenta praevia, and placenta praevia marginalis occurs three times more often than placenta praevia centralis.
Placenta praevia occurs more often in multiparous women than in primiparous women. According to E. B. Derankova, placenta previa occurs in 25.7% of primiparous women and 74.3% of multiparous women.
A low location of the placenta in multiparous women is observed twice as often as in primiparous women.
With age, the incidence of placenta previa increases, even in primigravidas; Between 20 and 30 years, placenta previa is especially common, which is explained by the highest frequency of births in this period.
Sometimes placenta previa occurs several times in a row in the same woman.
Thus, placenta previa contributes to the occurrence of abnormal position and presentation of the fetus. The tone of the uterus in these cases is usually reduced, while with a normal (corporal) location of the placenta, only a “local” decrease in the tone of the uterus is observed at the location of the placenta.
Some authors attribute the reasons for the location of the fertilized egg in the lower segment and in the lumen of the cervical canal due to the fertilized egg itself, since the latter plays an active role in implantation, others - due to morphological changes in uterine tissue.
This includes primarily atrophic and dystrophic processes in the uterine mucosa. The condition after excessive curettage of the mucous membrane during abortion, atrophy of the mucous membrane during various processes of a general and local nature, hypoplasia of the uterus due to infantility, malnutrition of the mucous membrane in elderly primiparas - all these are reasons predisposing to abnormal location and attachment of the placenta. According to some authors, abortion has a prominent place among the causal factors. M.V. Florov believes that the frequency of placenta previa increases with the number of abortions.
Various chemical effects on the uterine mucosa, used to prevent pregnancy (lubricating the uterus with iodine tincture and other substances), also play a significant role in the occurrence of placenta previa. Inflammatory changes in the uterine mucosa due to gonorrhea, syphilis and others can also lead to atypical implantation of the fertilized egg.
Other changes in the mucous membrane of the uterus also lead to the slipping of the egg into the lower parts of the uterus: disappearance of folding, hypersecretion, disruption of the ciliary movements of the epithelial cilia. Parenchymal changes in the uterus, characterized by partial replacement of muscle fibers with connective tissue, are of known importance. These changes may be a consequence of frequent childbirth with a complicated course of the postpartum period or excessive distension of the uterus during multiple pregnancies and polyhydramnios.
Changes in the uterine mucosa and its unpreparedness to receive the fertilized egg also lead to the fact that villi can penetrate not only to the muscles, but even deeper - between the muscle bundles of the uterus, which is explained by a change in the enzymatic activity of the chorionic epithelium and a decrease in the reactive properties of the decidual tissue (E . I. Magracheva). Ingrowth of chorionic villi in the direction of the external os promotes eccentric narrowing of the lumen of the cervix.
Even germination of the entire uterine wall with penetration of villi into the parametria was observed (M.V. Elkin). In this case, not only placenta praevia centralis arises, but also placenta praevia accreta partialis.
Among the predisposing factors, it is necessary to note diseases of the kidneys, heart and liver. Congestion that occurs as a result of diseases of these organs causes changes in the uterus that disrupt favorable conditions for implantation and development of the egg.
However, in the occurrence of placenta praevia, not only the primary implantation of the egg in the area of the internal os or above it, but also the secondary spread of placental growth to the lower segment (with normal implantation) may be important.
The placenta sometimes reaches a large size and can extend from the fundus to the cervix; often in such cases it is very thin and not typically round, but has tongue-like protrusions. The “presenting” placenta differs morphologically from the normally located one in that the attachment of the umbilical cord is almost always lateral or even marginal, the thickness of the placenta is less, and its area is much larger than normal.
Location of the placenta: norm and pathology, causes of anomalies, symptoms and possible complications, diagnosis and treatment. Childbirth and precautions
The placenta is an organ located in the uterus and functions only during pregnancy. It is thanks to him that the normal development of pregnancy until birth becomes possible, so it is important that the placenta “works” normally. In this case, not only the correct structure of the placenta matters, but also its correct location. Placenta previa is a serious complication of pregnancy, which, fortunately, does not occur very often.
The placenta is laid at the very beginning of pregnancy and is fully formed. It provides nutrition to the fetus, removes metabolic products, and also performs the function of the lungs for it, because It is through the placenta that the fetus receives the oxygen necessary for its life. In addition, the placenta is a real “hormonal factory”: hormones are formed here that ensure the preservation and normal development of pregnancy, the growth and development of the fetus.
The placenta consists of villi - structures within which blood vessels pass. As pregnancy progresses, the number of villi, and therefore the number of vessels, constantly increases.
Location of the placenta: norm and pathology
On the side of the uterus, at the placenta attachment site, there is a thickening of the inner membrane. In it, depressions are formed that form the intervillous space. Some villi of the placenta grow together with the maternal tissues (they are called anchor), while the rest are immersed in maternal blood, filling the intervillous space. The anchor villi of the placenta are attached to the septa of the intervillous spaces; vessels that carry arterial maternal blood, saturated with oxygen and nutrients, pass through the thickness of the septa.
The placental villi secrete special substances - enzymes that “melt” small arterial vessels carrying maternal blood, as a result of which blood flows from them into the intervillous space. It is here that the exchange takes place between the blood of the fetus and the mother: with the help of complex mechanisms, oxygen and nutrients enter the blood of the fetus, and metabolic products of the fetus enter the blood of the mother. The fetus is connected to the placenta using the umbilical cord. One end of it is attached to the umbilical region of the fetus, the other to the placenta. Inside the umbilical cord there are two arteries and a vein, carrying blood from the fetus to the placenta and back, respectively. Blood rich in oxygen and nutrients flows through the umbilical cord vein to the fetus, and venous blood from the fetus, containing carbon dioxide and metabolic products, flows through the arteries.
Normally, the placenta is located closer to the fundus of the uterus along the anterior or, less commonly, posterior wall. This is due to more favorable conditions for the development of the fertilized egg in this area. The mechanism for choosing the place of attachment of the fertilized egg is not completely clear: there is an opinion that gravity plays a role in choosing the place - for example, if a woman sleeps on her right side, then the egg is attached to the right wall of the uterus. But this is just one theory. What can be said with certainty is that the fertilized egg does not attach to unfavorable places for this, for example, to the location of myomatous nodes or to places where the inner lining of the uterus is damaged as a result of previous curettages. Therefore, there are other options for the location of the placenta, in which the placenta is formed closer to the lower part of the uterus. There are low-lying placenta and placenta previa.
The placenta is said to be low when its lower edge is located at a distance of no more than 6 cm from the internal os of the cervix. This diagnosis is usually made during an ultrasound. Moreover, in the second trimester of pregnancy, the frequency of this pathology is approximately 10 times higher than in the third trimester. It's quite simple to explain. Conventionally, this phenomenon is called “migration” of the placenta. In fact, the following happens: the tissues of the lower part of the uterus, which are very elastic, undergo significant stretching and are pulled upward as the duration of pregnancy increases. As a result of this, the lower edge of the placenta seems to move upward, and as a result, the location of the placenta becomes normal.
Placenta previa is a more serious diagnosis. In Latin this condition is called placenta praevia. "Pre via" literally means before life. In other words, the term “placenta previa” means that the placenta is on the way to giving birth to new life.
Placenta previa can be complete or central, when the entire placenta is located in the lower part of the uterus and completely covers the internal os of the cervix. In addition, partial placenta previa occurs. This includes marginal and lateral presentation. A lateral placenta previa is said to occur when up to 2/3 of the uterine outlet is covered by placental tissue. With marginal placenta previa, no more than l/3 openings are closed.
Causes of anomalies
The main cause of placental attachment abnormalities is changes in the inner wall of the uterus, as a result of which the process of attachment of the fertilized egg is disrupted.
These changes are most often caused by the inflammatory process of the uterus, which occurs against the background of curettage of the uterine cavity, abortion, or associated with sexually transmitted infections. In addition, deformation of the uterine cavity, caused either by congenital anomalies of the development of this organ or acquired causes - uterine fibroids (benign tumor of the uterus), predisposes to the development of such placental pathology.
Placenta previa can also occur in women suffering from serious diseases of the heart, liver and kidneys, as a result of congestion in the pelvic organs, including the uterus. That is, as a result of these diseases, areas in the wall of the uterus appear with worse blood supply conditions than other areas.
Placenta previa in multiparous women occurs almost three times more often than in women carrying their first child. This can be explained by the “baggage of diseases,” including gynecological ones, that a woman acquires at the age of her second birth.
There is an opinion that this pathology of the location of the placenta may be associated with a violation of some functions of the fertilized egg itself, as a result of which it cannot attach to the most favorable area of the uterus for development and begins to develop in its lower segment.
Watch out for bleeding!
Bleeding with placenta previa has its own characteristics. It is always external, i.e. the blood flows out through the cervical canal, rather than accumulating between the wall of the uterus and the placenta in the form of a hematoma.
Such bleeding always begins suddenly, as a rule, without any visible external cause, and is not accompanied by any pain. This distinguishes them from bleeding associated with premature termination of pregnancy, when, along with bloody discharge, there is always cramping pain.
Often bleeding begins at rest, at night (I woke up “in a pool of blood”). Once occurring, bleeding always recurs, with greater or lesser frequency. Moreover, you can never predict in advance what the next bleeding will be in terms of strength and duration.
Afterwards, such bleeding can be provoked by physical activity, sexual intercourse, any increase in intra-abdominal pressure (even coughing, straining, and sometimes an examination by a gynecologist). In this regard, an examination in a chair of a woman with placenta previa should be carried out in compliance with all precautions in a hospital setting, where emergency assistance can be provided in the event of bleeding. The bleeding itself is dangerous for the life of mother and baby.
Quite often, placenta previa can be combined with its tight attachment, as a result of which independent separation of the placenta after childbirth becomes difficult.
It should be noted that the diagnosis of placenta previa, with the exception of its central variant, will be quite correct only closer to childbirth, because the position of the placenta may change. This is all connected with the same phenomenon of “migration” of the placenta, due to which, when the lower segment of the uterus is stretched at the end of pregnancy and during childbirth, the placenta can move away from the area of the internal os and not interfere with normal childbirth.
Symptoms and possible complications
The main complications and the only manifestations of placenta previa are spotting. Depending on the type of presentation, bleeding may occur for the first time during various periods of pregnancy or childbirth. Thus, with central (complete) placenta previa, bleeding often begins early - in the second trimester of pregnancy; with lateral and marginal variants - in the third trimester or directly during childbirth. The severity of bleeding also depends on the type of presentation. With complete presentation, bleeding is usually more profuse than with incomplete presentation.
Most often, bleeding appears during pregnancy, when the preparatory activity of the lower segment of the uterus is most pronounced. But every fifth pregnant woman diagnosed with placenta previa notes the appearance of bleeding in the early stages (16-28 weeks of pregnancy).
What is the cause of bleeding during placenta previa? During pregnancy, the size of the uterus constantly increases. Before pregnancy, they are comparable to the size of a matchbox, and by the end of pregnancy, the weight of the uterus reaches 1000 g, and its dimensions correspond to the size of the fetus along with the placenta, amniotic fluid and membranes. This increase is achieved mainly due to an increase in the volume of each fiber that forms the wall of the uterus. But the maximum change in size occurs in the lower segment of the uterus, which stretches more as the due date approaches. Therefore, if the placenta is located in this area, then the process of “migration” proceeds very quickly, the low-elastic tissue of the placenta does not have time to adapt to the rapidly changing size of the underlying uterine wall, and placental abruption occurs over a greater or lesser extent. At the site of detachment, damage to blood vessels occurs and, accordingly, bleeding.
With placenta previa, there is often a threat of miscarriage: increased uterine tone, pain in the lower abdomen and lumbar region. Often, with this location of the placenta, pregnant women suffer from hypotension - a persistently reduced blood pressure. A decrease in pressure, in turn, reduces performance, causes weakness, a feeling of weakness, and increases the likelihood of fainting and headaches.
In the presence of bleeding, anemia is often detected - a decrease in the level of hemoglobin in the blood. Anemia can aggravate the symptoms of hypotension, and oxygen deficiency caused by decreased hemoglobin levels adversely affects fetal development. Growth retardation and fetal growth restriction syndrome (FGR) may occur. In addition, it has been proven that children born to mothers who suffered from anemia during pregnancy always have a reduced hemoglobin level in the first year of life. And this, in turn, reduces the baby’s body’s defenses and leads to frequent infectious diseases.
Due to the fact that the placenta is located in the lower segment of the uterus, the fetus often takes an incorrect position - transverse or oblique. Often there is also a breech presentation of the fetus, when its buttocks or legs are facing the exit from the uterus, and not the head, as usual. All this makes it difficult or even impossible to give birth to a child naturally, without surgery.
Diagnosis of placenta previa
Diagnosis of this pathology is most often not difficult. It is usually installed in the second trimester of pregnancy based on complaints of periodic bleeding without pain.
During an examination or ultrasound, a doctor may reveal an abnormal position of the fetus in the uterus. In addition, due to the low location of the placenta, the underlying part of the child cannot descend into the lower part of the uterus, therefore a characteristic feature is also the high standing of the presenting part of the child above the entrance to the pelvis. Of course, modern doctors are in a much better position compared to their colleagues 20-30 years ago. At that time, obstetricians-gynecologists had to navigate only by these signs. After the introduction of ultrasound diagnostics into widespread practice, the task became significantly simplified. This method is objective and safe; Ultrasound allows you to get a high degree of accuracy about the location and movement of the placenta. For these purposes, three-time ultrasound control is advisable at 16, 24-26 and at. If an ultrasound examination does not reveal a pathology in the location of the placenta, the doctor may, upon examination, identify other causes of bleeding. They can be various pathological processes in the vagina and cervix.
Observation and treatment of placenta previa
An expectant mother diagnosed with placenta previa needs careful medical supervision. The timely conduct of clinical trials is of particular importance. If even a slightly reduced level of hemoglobin or disorders in the blood coagulation system are detected, the woman is prescribed iron supplements, because in this case, there is always a risk of rapid development of anemia and bleeding. If any, even minor, deviations in health are detected, consultation with relevant specialists is necessary.
Placenta previa is a serious pathology, one of the main causes of serious obstetric hemorrhage. Therefore, if bleeding develops, all the health problems a woman has, even minor ones, can aggravate her condition and lead to adverse consequences.
Mode plus diet
If there is no bleeding, especially with partial placenta previa, the woman can be observed on an outpatient basis.
In this case, it is recommended to follow a gentle regimen: physical and emotional stress should be avoided, and sexual contact should be excluded. You need to sleep at least 8 hours a day and spend more time in the fresh air.
The diet must contain foods rich in iron: buckwheat, beef, apples, etc. There must be sufficient protein content, because without it, even with a large intake of iron into the body, hemoglobin will remain low: in the absence of protein, iron is poorly absorbed. It is useful to regularly eat fiber-rich vegetables and fruits, because... Retention of stool can provoke the appearance of bloody discharge. Laxatives are contraindicated for placenta previa. Like all pregnant women, patients with placenta previa are prescribed special multivitamin preparations. If all these conditions are met, the manifestations of all the symptoms described above, which accompany placenta previa in most cases, are reduced, which means that conditions are provided for the normal growth and development of the child. In addition, in the event of bleeding, the adaptive capabilities of the woman’s body increase, and blood loss is more easily tolerated.
In the presence of bloody discharge, observation and treatment of pregnant women with placenta previa during pregnancy beyond this period is carried out only in obstetric hospitals that have the conditions for providing emergency care in an intensive care unit. Even if the bleeding has stopped, the pregnant woman remains under the supervision of hospital doctors until the due date.
In this case, treatment is carried out depending on the strength and duration of bleeding, the duration of pregnancy, and the general condition of the woman and fetus. If the bleeding is minor, the pregnancy is premature and the woman feels well, conservative treatment is carried out. Strict bed rest and medications to reduce uterine tone and improve blood circulation are prescribed. If anemia is present, a woman takes medications that increase hemoglobin levels and general health-improving medications. Sedatives are used to reduce emotional stress.
Childbirth
In case of complete placenta previa, even in the absence of bleeding, a cesarean section is performed at 38 weeks of pregnancy, because Spontaneous birth is impossible in this case. The placenta is located on the path of the baby’s exit from the uterus, and if an attempt is made to give birth on its own, its complete detachment will occur with the development of very severe bleeding, which threatens the death of both the fetus and the mother.
The operation is also used at any stage of pregnancy if the following conditions are present:
- placenta previa, accompanied by significant bleeding, life-threatening;
- repeated bleeding with anemia and severe hypotension, which are not eliminated by the prescription of special medications and are combined with impaired fetal condition.
A cesarean section is routinely performed when partial placenta previa is combined with another pathology, even in the absence of bleeding.
If a pregnant woman with partial placenta previa carries the pregnancy to term, in the absence of significant bleeding, it is possible that the birth will occur naturally. When the cervix is dilated by 5-6 cm, the doctor will finally determine the variant of placenta previa. With a small partial presentation and minor bleeding, the amniotic sac is opened. After this manipulation, the fetal head descends and compresses the bleeding vessels. The bleeding stops. In this case, it is possible to complete the birth naturally. If the measures taken are ineffective, the birth is completed promptly.
Unfortunately, after the baby is born, there remains a risk of bleeding. This is due to a decrease in the contractility of the tissues of the lower segment of the uterus, where the placenta was located, as well as the presence of hypotension and anemia, which were already mentioned above. In addition, it has already been said about the frequent combination of previa and tight attachment of the placenta. In this case, after childbirth, the placenta cannot completely separate from the walls of the uterus on its own, and a manual examination of the uterus and separation of the placenta must be performed (the manipulation is carried out under general anesthesia). Therefore, after giving birth, women who have had placenta previa remain under the close supervision of hospital doctors and must carefully follow all their recommendations.
Infrequently, but there are still cases when, despite all the efforts of doctors and a cesarean section, the bleeding does not stop. In this case, you have to resort to removing the uterus. Sometimes this is the only way to save a woman's life.
Precautionary measures
It should also be noted that with placenta previa, you should always keep in mind the possibility of severe bleeding. Therefore, it is necessary to discuss with your doctor in advance what to do in this case, which hospital to go to. Staying home, even if the bleeding is light, is dangerous. If there is no prior agreement, you need to go to the nearest maternity hospital. In addition, with placenta previa, it is often necessary to resort to a blood transfusion, so if you have been diagnosed with this, find out in advance which relative has the same blood type as you, and get his consent to donate blood for you if necessary (the relative must get tested for HIV, syphilis, hepatitis in advance).
You can arrange at the hospital where you will be observed so that your relatives donate blood for you in advance. At the same time, it is necessary to obtain a guarantee that the blood will be used specifically for you - and only if you do not need it will it be transferred to a general blood bank. It would be ideal for you to donate blood for yourself, but this is only possible if your condition is not alarming, all indicators are normal and there is no bleeding. It is possible to donate blood for storage several times during your pregnancy, but you also need to ensure that your blood is not used without your knowledge.
Although placenta previa is a serious diagnosis, modern medicine allows you to carry and give birth to a healthy child, but only if this complication is diagnosed in a timely manner and with strict adherence to all doctor’s prescriptions.
When everything is over and you and your baby find yourself at home, try to properly organize your life. Try to get more rest, eat right, and be sure to take your baby for walks. Don't forget about multivitamins and medications to treat anemia. If possible, do not give up breastfeeding. This will not only lay the foundation for the baby’s health, but will also speed up the recovery of your body, because... Stimulation of the nipple through sucking causes the uterus to contract, reducing the risk of postpartum bleeding and inflammation of the uterus. It is advisable that at first you have someone to help you with child care and household chores, because your body has gone through a difficult pregnancy and needs to recover.
Evgenia Nazimova
obstetrician-gynecologist, Moscow
12/17/2007 00:07:52, Olga
Doctors do not like this diagnosis and try to convince her to terminate the pregnancy at the very beginning, when the first ultrasound confirmed the presentation. and they don’t say that everything can change. I liked the article, detailed, necessary, at one time I collected bit by bit any information about this complication. In conclusion, the article is very optimistic. very necessary words about the opportunity to give birth to a healthy child no matter what. I want another child and hope that this complication does not tend to recur.
The article is interesting, but it leaves no hope for women with previa that the placenta will return to its normal position by 30 weeks. I had bleeding at 22 weeks, the diagnosis was complete presentation. So, after a month, the placenta rose 6 cm from the internal os (the lower limit of normal). So I would like to say that presentation is not a final diagnosis at the beginning of the 2nd trimester and it is not necessary to go to the hospital before birth.
07/10/2006 13:21:58, Katyusha– a complication of pregnancy, which is characterized by the localization of the baby’s place in the lower segment of the uterus, closer than 6 cm from its internal os. The danger is that the anomaly does not manifest itself in any way. It is possible to determine the low location of the placenta only during an ultrasound scan or if complications develop - damage, organ detachment, accompanied by pathological signs. Treatment is carried out on an outpatient basis; a protective regime and drug therapy are indicated. In most cases, with a low-lying placenta, delivery is carried out by cesarean section.
As a rule, a low location of the placenta is detected during ultrasound screening of the first trimester, but closer to the 20th week, in approximately 70% of cases, migration of the child's place occurs, and the diagnosis is removed. By the end of pregnancy, this pathology persists in only 5% of patients. If a low location of the placenta is detected in the third trimester, the likelihood of it moving is extremely low.
Causes
Scientists have still not been able to definitively establish the reasons for the low location of the placenta. However, based on numerous studies, it has been suggested that abnormal attachment of the child’s place occurs against the background of diffuse hyperplasia of the chorionic villi and marginal death of individual elements of the decidua. Thinning of the myometrium, which has developed as a result of numerous abortions, curettage and other gynecological manipulations, can cause such changes and lead to a low location of the placenta. The risk of obstetric anomalies increases against the background of previous miscarriages, inflammatory and infectious diseases of the reproductive organs.
A low-lying placenta is often diagnosed after a cesarean section as a result of scar formation on the uterus. Pathology is more likely to develop during multiple pregnancies, if a woman has a history of 3 or more births, against the background of benign diseases, for example, fibroids. Congenital anomalies of the uterus, in particular, a bicornuate or saddle-shaped uterus, the presence of septa in the organ cavity, also increase the possibility of a low-lying placenta. The high-risk group includes patients prone to bad habits, exposed to stress, and performing heavy physical work.
Classification
In obstetrics, two types of low placenta are diagnosed depending on the location of the embryonic organ in relation to the uterus itself. Based on this criterion, the pregnancy prognosis can also be different. The following forms of anomaly are distinguished:
- Low location of the placenta on the posterior wall of the uterus. This is a more favorable option for the development of pathology. As the uterus increases in size, migration of the baby's place often occurs. Accordingly, space is freed up for the child, and childbirth is highly likely to occur through natural means.
- Low location of the placenta on the anterior wall of the uterus. It is diagnosed quite rarely, but has an unfavorable prognosis. If, when the baby's place is localized on the back wall, it tends to move upward, then in this case, as the uterus enlarges, the placenta will “move” downward. In this case, there is a threat of partial or complete blocking of the uterine os. The anterior low location of the placenta often causes umbilical cord entanglement, fetal hypoxia, and premature placental abruption.
Symptoms of low placenta
Clinically, a low location of the placenta in most cases does not manifest itself. Women usually feel well, and abnormal attachment of the baby’s place can be detected during a routine obstetric ultrasound. A low location of the placenta may be accompanied by pathological symptoms if complications begin to develop against its background. With premature detachment, nagging pain in the abdomen, sacrum, and bleeding are possible. It is extremely rare that this diagnosis contributes to the development of late toxicosis. In addition, a low location of the placenta in late gestation can lead to fetal hypoxia. Oxygen deficiency is manifested by a decrease in the child’s motor activity, rapid or slow heartbeat.
Diagnosis and treatment
It is possible to identify a low location of the placenta during ultrasound screening of the 1st, 2nd or 3rd trimester of pregnancy, which is routinely prescribed by an obstetrician-gynecologist to all patients at 12, 20 and 30 weeks of pregnancy, respectively. Determining the abnormal attachment of the baby's place in the early stages is not critical, since closer to the middle of gestation it migrates and takes the correct position without risk to the health of the woman or the fetus. Ultrasound at a low location shows not only its exact location, but also its thickness, the level of blood flow in the vessels, and the condition of the fetus. Evaluation of these parameters allows us to suspect more serious complications, in particular, hypoxia, entanglement, and incipient detachment.
Treatment for low placenta depends on the gestational age, as well as the general condition of the woman and fetus. Detection of an anomaly in the first trimester does not require additional therapy; it is enough to limit physical activity. It is highly likely that the baby's place migrates as the uterus increases in volume. Hospitalization for low-lying placenta is indicated when there is a threat of premature abruption, severe fetal hypoxia, or closer to birth in the period of 35-36 weeks to examine the patient and determine the delivery plan.
A low location of the placenta requires correction of the daily routine. The patient should rest as much as possible. It is important to completely exclude psycho-emotional and physical stress, sexual contact, as all this can provoke complications in the form of detachment. If the placenta is low, you should walk less and avoid traveling on public transport. It is recommended to rest in a lying position, while raising the leg end to increase blood flow to the pelvic organs, in particular to the uterus and placenta.
Drug treatment for low-lying placenta is not prescribed. Management of pregnancy in this case requires more careful monitoring; most likely, consultation with an obstetrician-gynecologist will be prescribed more often than usual. Correction of the condition of the patient or fetus is carried out only if there is a threat or development of complications against the background of abnormal attachment. When placental abruption begins, the use of drugs that improve blood flow in the vessels of the umbilical cord and vitamin complexes is indicated. If uterine hypertonicity is present against the background of a low placenta, tocolytics are used.
With a low location of the placenta, delivery is possible both through the vaginal genital tract and by cesarean section. The first option is possible if the baby's seat is placed no lower than 5-6 cm from the internal os of the uterus, as well as good condition of the mother and fetus, sufficient maturity of the cervix and active labor. A planned cesarean section is performed when a low location of the placenta is accompanied by the threat of premature detachment, with severe fetal hypoxia.
Prognosis and prevention
The vast majority of pregnancies occurring with a low-lying placenta have a favorable outcome. In 70% of patients with this diagnosis, closer to childbirth, the baby's place takes the correct position on the anterior or posterior wall of the uterus. In other cases, timely diagnosis and the appointment of a protective regime make it possible to avoid complications, carry the pregnancy to 38 weeks and give birth to an absolutely healthy child. In 40% of women with a low-lying placenta, birth is carried out by caesarean section. In other cases, children are born through the natural birth canal. Sometimes the fetus shows signs of intrauterine hypoxia.
Prevention of low placenta consists of early diagnosis and treatment of gynecological abnormalities that contribute to thinning of the uterine mucosa. Women should also avoid abortions and register their pregnancy with an obstetrician-gynecologist in a timely manner. Avoiding stress and physical activity after conception will help reduce the likelihood of developing a low-lying placenta. You should also avoid working in hazardous enterprises, give up bad habits, get plenty of rest and ensure a sufficient supply of nutrients to the expectant mother’s body. Walking in the fresh air has a positive effect on the health of the woman and the fetus. Each patient must follow all the recommendations of the obstetrician-gynecologist, take the necessary tests and conduct screening studies in order to detect a low-lying placenta as early as possible and begin therapy.
The placenta is the most important organ for supporting the vital functions of the embryo. It is through it that nutrients and oxygen enter, and waste products are eliminated. The placenta serves as a protective barrier against infections and viruses.
Not every woman knows about all the features of pregnancy and how the process of conception and formation of an embryo occurs. Often, the diagnosis of improper attachment of the placenta makes you panic. How should the organ be attached normally? What to do if the location of the placenta is incorrect? What is presentation? What does the diagnosis of “low placentation” mean?
The optimal place for the placenta to attach
The placenta, or baby's place, ensures the safety of the fetus, so the optimal zone of its attachment should be safe. From a physiological point of view, such a place is the fundus of the uterus or its posterior wall. As the baby grows, the uterus will stretch, but the back part will remain dense.

Hence there are several advantages:
- the placenta remains motionless, in this position its descent practically does not occur;
- with the tone of the uterus and its contractions, the placenta is not affected, and the risk of its detachment is reduced;
- the child’s movements have minimal impact on the child’s seat;
- the risk of damage to the placenta due to abdominal injuries is reduced;
- the likelihood of bleeding during childbirth is reduced.
Reasons for incorrect localization of a child's seat
Cases when the baby's place is attached to the side walls of the uterus are not uncommon. This is not scary; such attachment is not considered pathological. Anterior placenta previa, or more precisely, its attachment to the anterior wall (see photo) requires more careful observation. Low attachment is considered especially unfavorable, when the internal os is partially or completely blocked.

Reasons for attachment of the fertilized egg to the anterior wall of the uterus or close to the uterine os:
- inflammatory processes or operations on the uterus that have changed its inner layer;
- endometriosis of the cervix (hormonal disease characterized by proliferation of the mucous membrane of the organ);
- myoma (fibroids) of the uterus (benign tumor);
- multiple pregnancy;
- pathology of the uterus (inverted or curved uterus);
- numerous births;
- presence of a cesarean section scar;
- history of abortion;
- The woman is over 40 years old.
The cause of the pathology is not only the health status of the mother, but also the delay in the development of the fertilized egg. Sometimes the egg does not have time to attach to the endometrium in time. As a result, it clings to the front wall or descends to the lower parts of the organ, where it remains.
Features of the course of pregnancy and childbirth
A placenta on the anterior wall is not a death sentence. Modern doctors do not consider such a diagnosis to be a pathology. It matters how high the placenta is located from the os of the uterus. Low fastening, especially on the front side, is fraught with miscarriage.
Incorrect position of the baby's place is diagnosed at the first planned ultrasound. The height of its location changes; a low mount is fixed in the first or second trimester. Next, the uterus stretches and the placenta begins to migrate. By the third trimester of pregnancy, only 3% of women still have the problem.
When attached to the back wall
The placenta on the posterior wall of the uterus is the most physiologically correct option for its location. It is not subject to stretching or external influence, which ensures the safety of both the fetus and the protective organ itself. The risk of placental abruption in this location is minimal.

When the placenta is localized on the posterior wall, the cervix of the uterus is not blocked by anything. If the baby is in the correct position before birth (head down), there are no other contraindications, the birth takes place naturally. The risk of complications during them is minimized.
If the placenta is attached to the anterior wall
With anterior attachment of the placenta, they speak of an unfavorable option. The organ is located in the part of the uterus that is greatly stretched. The placenta is not so elastic, and there is a high risk of detachment. With such a localization, it is very difficult to listen to the baby’s heartbeat and perform palpation; fetal movements may not be felt. For research you will have to use ultrasound.
Women with an anterior (especially low) position of the baby's place need to be especially careful, since any abdominal injuries threaten placental abruption and premature birth. When combined with a breech or lateral presentation, a natural birth may not be possible.
It is impossible to change the incorrect location of the placenta; at best, it rises on its own as the fetus grows. However, this situation requires constant monitoring. The condition of the baby and mother is monitored throughout pregnancy. Attachment of the placenta to the anterior wall threatens bleeding - which means blood tests will be required for coagulation and hemoglobin levels. It is important to prevent the development of anemia.
If bleeding occurs before 24 weeks, the woman is hospitalized. Depending on the severity of blood loss, a decision is made to terminate or continue the pregnancy. In the latter case, the expectant mother is prescribed complete rest, she is left in the hospital, and conservation therapy is prescribed. The main task of doctors in this case is to extend the pregnancy until the child becomes viable. Next, a caesarean section is performed.

With lateral attachment
Lateral attachment of the placenta on the right or left side is not uncommon. It is important for doctors to monitor whether the baby's place is blocking the exit from the uterus. This is done using ultrasound. Often the decision to manage labor is made after it has begun. After the cervix opens 4 centimeters or more, an examination is performed. If the uterine os is blocked, the fetal membranes and the placenta or part thereof are visible during an ultrasound examination.
Symptoms, types and dangers of low placentation
Low placentation is a pathology that does not have any symptoms at an early stage. Only in the later stages may a woman notice nagging pain in the lower abdomen and the appearance of blood. By this time, with constant monitoring, the problem has already been identified. The location of the placenta is visible on the first planned ultrasound, then the dynamics of its migration are monitored.
There are 4 degrees of presentation:
- the child seat is attached from below at a distance of less than 3 cm from the internal pharynx;
- the placenta is localized near the internal os, but does not block the baby’s exit;
- the lower part of the organ covers the pharynx, the center and top are localized at the top and bottom of the uterus, the location is asymmetrical;
- the exit is completely blocked by the main part of the placenta, its edges are attached to the walls of the uterus.

Low placentation can be characterized by fastening of the baby's place along the posterior or anterior wall of the uterus. The difference is that in the first case the prognosis is more favorable - the localization of the placenta may change to a higher one. In the second case, as the fetus grows, the placenta will most likely sink even lower, which can lead to the following complications:
- overlap of the uterine os;
- incorrect position of the fetus, entanglement of the umbilical cord;
- fetal hypoxia;
- premature placental abruption;
- risk of bleeding during childbirth.
There are risks for women too. During the expulsion of the placenta, the pregnant woman does not always feel discomfort; the blood may not come out, but may remain in the uterine cavity. Uteroplacental apoplexy occurs. In this case, an urgent caesarean section is necessary, the uterus is completely removed. Untimely assistance threatens the woman’s life.

Is it possible to influence the location of the placenta?
It is impossible to have a direct influence on the location of the child's place, but it is possible to minimize the indirect causes of the development of pathologies. Measures to prevent low, anterior attachment or placenta previa include:
- exclusion of abortion;
- timely treatment of gynecological diseases;
- early registration for pregnancy;
- eliminating stress and physical activity in the early stages;
- healthy lifestyle: maintaining good physical shape, proper nutrition, walking in the fresh air;
- preparation for pregnancy: examination, taking vitamins.
All these factors not only improve the health of the expectant mother, but also make the embryo stronger and more resilient, and increase the likelihood of the correct location of the placenta. For most women, low placentation does not cause pregnancy complications, which means there is no need to panic. Localization of the baby's place at the bottom (central presentation) practically excludes the possibility of carrying a healthy baby. Timely diagnosis allows the baby to be carried to 38–39 weeks, after which a caesarean section is performed.
The placenta plays a very important role.
The success of childbirth depends on how it is located, so you should know what types of placenta previa are. It is through this that the baby is supplied with oxygen.
The importance of the placenta cannot be overestimated. How well the pregnancy will proceed largely depends on it. Her condition affects the health of the unborn baby and his life in general. If an expectant mother is diagnosed with a pathology related to the placenta, this can be very dangerous. For example, placenta previa is a reason for careful monitoring of the health of the woman and fetus.
The diagnosis of placenta previa comes as a real shock to many. This is a very dangerous pathology, but a lot depends on the type of illness. For example, posterior presentation is not considered a serious problem. If a doctor has identified a similar situation, this does not mean that big problems await the woman and child. If the doctor has diagnosed the location of the placenta on the posterior wall, this means that everything is in order.
The posterior wall of the uterus is the least susceptible to deformation during pregnancy. If the doctor has diagnosed that the placenta is located along the anterior wall, this means that things are somewhat worse, since it can stretch and become thinner, which leads to detachment and displacement. However, this does not always happen.
Low placentation is more dangerous. In this case, the placenta is attached near the pharynx, at a distance of less than six centimeters. In such a situation, placental prolapse can be even greater. This leads to complete or partial presentation. This happens quite often in medical practice, but statistics show that with low placentation, natural childbirth can take place without serious problems.
Partial presentation can be of two types: lateral and marginal placenta previa. In the first case, the internal gap is blocked. In this case, a significant part of the passage is blocked, that is, about two-thirds of the hole. With marginal presentation, overlap also occurs, but only by a third.
In itself, this position of the placenta does not mean anything good. However, with such a diagnosis, there is no need to panic, since in most cases everything falls into place before the baby is born. Experts say that normal birth with partial presentation is quite possible. However, it all depends on the complexity of the particular case.

Central or complete placenta previa is considered the most difficult, since with such a pathology the entire cervix of the uterus closes, which means that the child will not have the opportunity to come out naturally. This is very dangerous not only for the unborn baby, but also for his mother.
With complete presentation of the embryonic organ, significant distension of the uterus and placental abruption occur. Considering that the uterine tissue stretches much better than the placental tissue, the integrity of the blood vessels is disrupted, which threatens serious bleeding. Sometimes such trouble happens at the beginning of the third trimester. Bleeding may occur throughout the rest of the pregnancy. With a central presentation of the baby's place, the natural birth of a baby is impossible. The child is born by caesarean section.

Causes of pathology
Placenta previa during pregnancy occurs due to changes in the condition of the uterine mucosa, that is, the endometrial layer. Thus, the fertilized egg does not have the opportunity to attach itself where it is needed, that is, at the bottom. The fundus of the uterus is the most convenient place due to the fact that stretching is least noticeable here, which also allows the fetus to receive a good blood supply.
In some cases, when the mother has diseases associated with the cardiovascular system, the blood supply to the uterine fundus may be disrupted. The fertilized egg will have to find a suitable place to complete the implantation process.
The finished egg does not have the opportunity to attach to the right place even if the endometrium is damaged. All kinds of deformations on the lining of the uterus can form during an abortion. Women who have undergone such operations are at particular risk, and they experience placenta previa much more often.

In medical practice, there are also cases where the cause of improper implantation of the fertilized egg was not a problem in the mother’s reproductive system, but the poor development of the egg. If there is a noticeable deviation from the norm, the egg may not have enough strength to reach the uterine fundus. As a result, it is attached directly at the entrance, that is, in the area of the internal pharynx.
Symptoms of placenta previa
The main symptom of this pathology is severe bleeding. This, moreover, threatens serious troubles, since a large loss of blood is dangerous for both the unborn baby and the young mother. Bleeding occurs due to the fact that part of the placenta moves away from the wall of the uterus, which leads to damage to blood vessels. Each location of the placenta is characterized by its own bleeding. For example, with low placenta previa, internal bleeding is most often observed, which looks like a hematoma on the body. In most other cases, this is vaginal bleeding, which can be strong or weak, depending on the complexity of the pathology.
Partial presentation is most often characterized by fairly heavy bleeding, which begins in late pregnancy. If placentation is complete, a similar symptom is observed already in the second trimester.

The expectant mother should remember that bleeding during pregnancy can be caused by other factors. These include excessive physical activity, sexual intercourse, examinations by a gynecologist and increased uterine tone.
This symptom is very dangerous, since large blood loss for the expectant mother and fetus is unacceptable. If bleeding is not stopped in time, it can cause hypotension and anemia. For this reason, in the presence of placenta previa, a woman should be constantly under the constant supervision of specialists. If there is bleeding and the central location of the embryonic organ, the expectant mother is sent to the hospital at 24 weeks. This is a very serious case that requires auxiliary treatment. A certain percentage of pregnancies with this type of pathology end in fetal death.
Treatment of pathology
The location of the placenta on the posterior wall does not require treatment, since this is the ideal location. All other variants of presentation are serious anomalies that can be dangerous both for the unborn child and for the mother herself. However, drug treatment for this anomaly is unknown to modern medicine. The only thing that can help in this case is careful monitoring of the woman’s health. In such a situation, doctors have the opportunity to eliminate dangerous symptoms and associated ailments that could worsen the situation. When placenta previa occurs, it is necessary to neutralize the bleeding in time and relieve the tone of the uterus so as not to harm the fetus and the woman’s health. If marginal placenta previa is diagnosed at 20 weeks, you should not worry too much, since things can still change until the end of pregnancy.

Special medications are not prescribed for this pathology. Depending on the complexity of the situation, bed rest and hospitalization may be recommended.
How does childbirth take place?
Most often, the birth of a baby occurs in the usual way. However, much depends on the type of anomaly. The danger of this pathology lies in the fact that during contractions, complete detachment of the placenta cannot be ruled out, which leads to hypoxia of the child and loss of blood, which is extremely dangerous for the mother. In such a situation, a caesarean section is performed urgently.
If there is no bleeding, it is quite possible that the birth will be normal and no problems will arise. If the location of the placenta is diagnosed on the anterior or posterior wall, then no special problems should arise, but if central presentation of the baby is confirmed, the woman undergoes a cesarean section at 38 weeks of pregnancy.