How to improve blood circulation in the uterus during pregnancy. Disturbance of uteroplacental blood flow during pregnancy
Most women do not know about such a test as Doppler until the third trimester, and from that moment Doppler testing becomes a completely common procedure for pregnant women.
Doppler is one of the ultrasound diagnostic methods that allows you to assess the intensity of blood flow in various vessels, for example, in the vessels of the uterus and umbilical cord. It is most informative after the 30th week, but if there are deviations during pregnancy (for example, if the fetus is delayed in development), Doppler ultrasound can be prescribed earlier - starting from the 20th week.
Indications for Doppler
Adequate placental blood flow ensures normal pregnancy. Impaired blood flow can lead to intrauterine growth retardation (IUGR), therefore the main reason for prescribing Doppler ultrasound during pregnancy is precisely the discrepancy between the size of the baby’s body and/or organs and the norms.
It is not necessary that if blood flow is impaired, the child will lag behind in development, but the risk of an unfavorable course of pregnancy increases significantly. Well, and vice versa, if there is a suspicion of a developmental delay in the fetus, but the blood flow is not impaired, then in most cases this indicates that the woman is carrying a low-weight but healthy child.
Doppler ultrasound is also prescribed for:
- premature maturation of the placenta;
- pronounced oligohydramnios or polyhydramnios;
- umbilical cord abnormalities;
- Rhesus conflict;
- gestosis (late toxicosis, complicated by vomiting, severe swelling and increased blood pressure in a pregnant woman);
- the expectant mother has kidney disease, hypertension, diabetes;
- suspected chromosomal pathology;
- non-immune hydrops fetalis;
- uneven development of babies during multiple pregnancies (when there is a difference in their body weights of more than 10%).
If the fetus has heart problems, Doppler is performed together with CTG, the so-called Doppler echocardiography.
In case of fetoplacental insufficiency, Doppler measurements are carried out systematically every 2-3 weeks.
Also, if complications develop during a previous pregnancy, Doppler ultrasound may be prescribed during a subsequent pregnancy.
Preparing for the study and how it is carried out
Doppler testing in pregnant women is carried out according to indications, and is not a mandatory examination during the normal course of pregnancy. But more and more often, in antenatal clinics, all women, without exception, undergo Doppler ultrasound at 30-34 weeks to assess the condition of the fetus.
This procedure is painless and harmless to both mother and fetus. The principle of Doppler testing is the same as a regular ultrasound during pregnancy: a special Doppler sensor is moved across the abdomen, which is equipped with every modern ultrasound diagnostic device. Therefore, this type of research does not require special preparation.
Doppler– this is a visual assessment of blood flow (when an ophthalmologist observes a color and graphic image of blood flow velocity curves from the monitor screen).
Dopplerography– this is the same Doppler, only the readings are additionally recorded on a tape in order to monitor changes (improvement/deterioration) in blood flow after treatment.
Interpretation of Doppler measurements
Uterine arteries (a. uterina dextra - right and a. uterina sinistra - left uterine artery, respectively). The uzist must determine the nature of blood flow in both the left and right uterine arteries, because with gestosis it can be disrupted in only one artery. Thus, by assessing the blood flow in only one artery, one can give a false conclusion, which will negatively affect the health of the baby and the expectant mother.
There is a scientific theory that if blood flow is disrupted in only one (mainly the right) uterine artery, a woman has a high risk of developing late toxicosis (preeclampsia) with all the negative consequences.
With gestosis, the blood flow in the uterine artery is first disrupted, and as the situation worsens, the blood flow in the umbilical cord arteries deteriorates. Therefore, if blood flow in the uterine arteries is disrupted, it is necessary to periodically repeat Doppler to monitor the situation.
To assess blood flow in the uterine arteries, the resistance index (IR or RI) is calculated.

Often, pregnancy-induced hypertension develops due to impaired uterine blood flow. The expectant mother's body independently increases blood pressure to increase blood flow into the intervillous space. This is how the mother, without realizing it, helps the baby. Thus, it is necessary to improve blood flow and hypertension will disappear on its own.
Impaired blood flow in the uterine arteries is when the value of IR, PI or SDO is greater than normal.
The pulsation index (PI) of the uterine arteries should be within the following limits.

Indicators in the right and left uterine artery may differ slightly from each other. If both indicators are within normal limits, then this picture is not considered a negative phenomenon.
Deviation of blood flow indicators from the norm in two uterine arteries at once indicates a violation of the uteroplacental circulation. This situation requires specific treatment - move more (regularly go swimming or do gymnastics for pregnant women).
Violation of blood flow in only one uterine artery indicates an asymmetry of uteroplacental blood flow. If the pregnancy proceeds normally and the baby develops in accordance with the term, then the placenta is fulfilling its functions.
You should be aware that at 18-21 weeks there may be a temporary disruption of blood flow in the uterine arteries. This phenomenon is explained by the fact that the adaptive physiological process of cytotrophoblast invasion has not yet been completely completed. Therefore, if abnormalities are detected in the uterine arteries, a repeat Doppler ultrasound should be performed after 2-3 weeks, i.e. observe the blood flow over time.
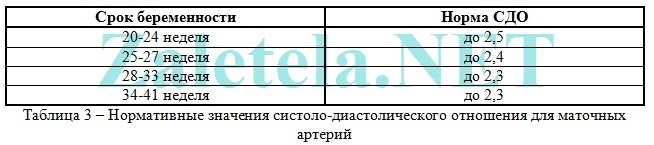
The systole-diastolic ratio (SDR) in the uterine arteries should be:
Umbilical cord arteries (a. umbilicalis). To obtain true results, the study should be carried out only while the baby is at rest, and only when his heart rate is between 120-160 beats per minute. After all, physiologically it is so laid down that when the heart rate increases, the IR in the umbilical cord artery decreases, and vice versa, when the heart rate decreases, the IR increases.
Measuring blood flow in the umbilical cord arteries should be done while the pregnant woman is lying on her back! Assessment of the severity of umbilical cord blood flow disturbance cannot be objective when the expectant mother is positioned “on her left side.”
The umbilical cord should have two arteries and one vein. If there is an anomaly (a single umbilical cord artery), then the fetus may suffer from a lack of oxygen and nutrients, which is why it lags behind in weight and growth. But it happens that the fetus adapts to such an existence and does not experience a deficiency of necessary substances. Such babies are born with low weight, but absolutely viable. Therefore, if there is one umbilical cord artery and the blood flow in it is not impaired, then there is no cause for concern. But if the blood flow in a single artery is impaired, inpatient treatment should be carried out to improve blood flow and, if necessary, early delivery (if the fetus is severely delayed in development).
The most widely used method for assessing the nature of blood flow in the umbilical cord arteries is the resistance index. The readings in both umbilical cord arteries should be almost the same.

Impaired blood flow in the umbilical cord is when the value of IR, PI or SDO in the umbilical cord arteries is higher than normal.
The pulsation index (PI or PI) of the umbilical cord arteries must meet the following standards:

Registration of zero and reverse values of diastolic blood flow is pathological. This means that the fetus is in critical condition.
There are only 2-3 days left from the moment permanent reverse values appear until the death of the fetus, so it is necessary to perform a caesarean section as soon as possible in order to save the baby’s life. This is only possible starting from week 28, when the baby is viable.
Systole-diastolic ratio (SDR) in the umbilical cord arteries:

If the blood flow in the umbilical cord is impaired, then, as a rule, fetal development is delayed. If there is no developmental delay now, but the blood flow in the umbilical cord is impaired, then without treatment, the fetus may experience developmental delay.
Middle cerebral artery of the fetus (a. cerebri media). When the fetus suffers, it is observed increase in the values of PI, SDO and speed in the SMA.

Maximum velocity (aka V max) in the fetal middle cerebral artery:

Systole-diastolic ratio (SDR) for the middle cerebral artery:

Fetal aorta. It emerges from the left ventricle of the heart, runs along the spine and ends in the lower abdomen, where the aorta divides into two iliac arteries, which provide blood supply to the human legs.
Abnormalities in the blood flow of the aorta can only be detected after 22-24 weeks of pregnancy.
Impaired blood flow is increasing the values of IR, PI and SDO. Critical (indicating fetal death) is considered registration of extremely low values until their complete disappearance.

Changes in the aorta characterize the severity of intrauterine fetal hypoxia.


Systole-diastolic ratio (SDR) for the fetal aorta:

Ductus venosus (DV). It is studied with enhanced Doppler assessment of blood flow.
During the study, it is necessary not to take into account episodes of hiccup-like respiratory movements of the child and active movement.
Indices are not used to assess the ductus venosus.
The diagnostic criterion for the pathological condition of the fetus is the presence negative or zero blood flow values during the phase of atrial contraction. Zero or reverse values are recorded for fetal malnutrition, congenital defects of the right heart, and non-immune fetal hydrops.
Even with critical blood flow in the umbilical cord arteries, but with preserved blood flow in the ductus venosus during the phase of atrial contraction, it is possible to extend gestation until the optimal time for childbirth.
Description of blood flow disorders and their treatment
1st degree
1 A degree– disturbance of blood flow in the uterine arteries, while in the umbilical cord blood flow remains normal.
This degree of blood flow disturbance is not dangerous for the fetus.
Drug treatment for this condition is ineffective. Doctors still prescribe therapy with Actovegin and Curantil. Don't see each other on occasion!
In fact, if blood flow in the uterine arteries is impaired, it is more advisable to simply walk more often in the fresh air (breathing deeply) + eat right + move more (hiking, special exercises for pregnant women, morning exercises, yoga, swimming). And don't sit at the computer for hours! That's all the treatment is.
1 B degree– disturbance of blood flow in the umbilical cord arteries, but hemodynamics in the uterine arteries are normal.
This degree of blood flow impairment requires the use of blood thinning drugs to avoid developmental delay and fetal hypoxia.
In this case, treatment is prescribed aimed at improving blood circulation (the drug Placenta compositum, Curantil or Trental). Actovegin is prescribed as an antihypoxant that improves oxygen supply to the fetus.
A blood test for clotting ability (coagulogram) is also prescribed. In case of increased blood clotting, it is necessary to take stronger blood-thinning drugs than Curantil (for example, heparin or a product containing acetylsalicylic acid).
Degree I of the disorder does not lead to fetal death. Systematic monitoring of the nature of blood flow is carried out (every 2 weeks) “plus” monitoring of fetal CTG (after 28 weeks of pregnancy). In addition, be sure to monitor the blood pressure of a pregnant woman.
2nd degree– simultaneous disturbance of blood flow in the uterine arteries and in the umbilical cord, which does not reach critical values (when blood flow is preserved in the venous duct).
In this condition, it is mandatory to prescribe drug treatment in a hospital, where round-the-clock monitoring of the condition of the fetus is provided. It is also necessary to monitor the state of blood flow by performing Doppler + CTG every 2 days.
In grade II, hemodynamic disturbances are rare, but cases of intrauterine mortality may occur.
3rd degree– critical disturbances of blood flow in the umbilical cord with intact or impaired blood flow in the uterine arteries. A critical violation is understood as registration of reverse diastolic blood flow or its absence at all.
The third degree of violation poses a danger to the child’s health, because in half of the cases the baby’s intrauterine death occurs. Therefore, if a 3rd degree of blood flow disorder is detected, it is necessary to urgently perform a cesarean section in order to save the baby’s life, because at this stage of the disorder, treatment is not effective.
Conservative (natural) childbirth in the 3rd degree can lead to perinatal death of the child.
The cost of Doppler ultrasound in a private clinic is about 1,200 rubles.
During pregnancy, it is very important to constantly monitor the condition of the mother and fetus and their performance of vital functions. One of the most significant studies is the analysis of blood flow in the arteries of the uterus, the woman’s umbilical cord, as well as in the aorta and cerebral vessels of the child.
Among the main causes of perinatal mortality and morbidity, disruption of uterine blood flow (uteroplacental and fetal placental) is not the least important.
Blood flow in the placenta
The placenta, in which the fetus is located, supplies it with nutrition and oxygen from the mother’s blood and removes metabolic products from the child’s body. It is this organ that unites two complex vascular systems - the maternal one, which connects the vessels of the uterus and the placenta, and the fetal one, which passes into the umbilical arteries and leads to the fetus.
The above-mentioned circulatory systems are separated by a membrane that does not allow the blood of the mother and child to mix. The placenta acts as a kind of barrier, resistant to many viruses and harmful substances.
In some cases, for completely different reasons, placental insufficiency may develop, which inevitably affects the performance of the trophic, metabolic, transport, endocrine and other vital functions of the placenta. In this condition, the metabolism between the body of mother and child deteriorates significantly, which is fraught with consequences.
Causes of uterine blood flow disorders
Poor circulation in the uterus can be caused by increased pressure, pneumonia, intrauterine infection and insufficient oxygen supply to the fetus ().
To diagnose the blood flow system in obstetric practice, three-dimensional ultrasound (Doppler) is used, with the help of which the vessels are visible in the so-called 3D (three-dimensional) image. With the help of this modern diagnostic method, there is a prospect of diagnosing retroplacental bleeding and assessing cardiac malformations by monitoring blood flow. This method is indispensable, since with its help you can see defects even in the smallest vessels that form the microvasculature, monitor the development and formation of intraplacental hemodynamics, and also control the amount of oxygen and nutrients that should enter the fetal body. New opportunities have opened up for the early detection of obstetric complications, and if correction or treatment is started without wasting time, then circulatory disorders and further associated pathologies can be practically avoided.
Hemodynamic disorders during pregnancy
Hemodynamic disorders are divided into three degrees of severity:
First degree includes two subspecies:
- 1A is a violation of uteroplacental blood flow, which is the mildest. Fetal-placental circulation is preserved. In most cases, this problem is caused by intrauterine infection;
- 1B - uteroplacental blood flow is preserved, while pathologies occur in the fetoplacental blood flow.
Second degree characterized by disturbances of both blood flow systems, but does not involve cardinal changes.
Third degree is that disruption of the uteroplacental circulation leads to defects in blood circulation at the utero-fetal level.
In the first degree of violations, due to timely detection and adequate treatment, cases of fetal death can be avoided. Perinatal mortality in the second degree is 13.3%, in the third - 46.7%. During this time, it was found that correction of placental insufficiency in patients with third-degree hemodynamic impairment was ineffective. In this case, perinatal mortality during conservative birth was 50%, while it helps to avoid losses. 35.5% of newborns are admitted to the intensive care unit with the first degree, 45.5% with the second, and 88.2% with the third.
Prevention of blood flow disorders during pregnancy
Every woman who wants to give birth to a child must remember that the mother’s condition is completely transmitted to the unborn baby. Therefore, in order for the fetus to develop without complications, she needs to make up her diet from food containing a maximum of vitamins, micro- and macroelements, as well as rich in the required amount of carbohydrates, proteins and fats. If a pregnant woman is not bothered by swelling, then fluid intake should be at least 1-1.5 liters.
It is important to monitor changes in body weight, since by the end of pregnancy the weight gain should not exceed 10 kg.
There are risk groups that require the use of drug prophylaxis, which promotes the interaction of the body systems of the fetus and mother and prevents dysfunction of the uteroplacental circulation.
Timely adjusted methods of labor management and drug therapy will help to significantly reduce perinatal morbidity and mortality. But a high risk of severe neurological complications cannot be ruled out.
Especially for Elena Zhirko
Pregnancy is accompanied by various changes in a woman’s body, which are aimed at the full development of the child. Many processes and systems adapt to new conditions of existence, and the woman notes the appearance of previously unknown sensations. Any expectant mother wants her baby to be born healthy, and naturally worries about his condition when any abnormalities are detected.
The main factor that supports intrauterine growth and development of the child is the uteroplacental-fetal blood flow (UPF). This is a comprehensive system that supports the normal course of pregnancy. If the blood flow in the uterus is disrupted, then they speak of placental insufficiency. It is dangerous primarily due to miscarriage, and there are also frequent other negative consequences of this pathology for the expectant mother and child.
The lack of blood flow through the placenta must be detected in time, and treatment measures cannot be delayed.
Causes
Hemodynamic disturbances between the fetus and the woman’s body are provoked by many factors. They affect the placenta both during its formation and in later stages of pregnancy. Accordingly, primary and secondary circulatory failure are distinguished. As a result, all functions of the placenta as a separate organ are disrupted: transport, metabolic, protective, immune and endocrine. This is caused by the following conditions:
- Tumors of the uterus.
- Structural anomalies.
- Genetic defects.
- Hormonal dysfunctions.
- Consequences of abortion.
- Late toxicosis.
- Infectious diseases.
- Atherosclerosis, thrombosis.
- Hypertonic disease.
- Diabetes.
- Diseases of the thyroid gland and adrenal glands.
Most often, a woman has an underlying risk factor that can cause placental insufficiency. A combination of several similar conditions is often observed when carrying a child.
To identify the causes of placental blood flow disturbances, it is necessary to conduct periodic screenings at various stages of pregnancy.
Symptoms

Each pathology has its own clinical picture, which allows us to make a preliminary conclusion. Hemodynamic insufficiency is manifested by changes in all functions of the placenta, and as a result, mainly the fetus suffers. It receives all nutrients and oxygen in insufficient quantities, and the excretion of metabolic products may slow down. Signs of fetal hypoxia appear, which subsequently leads to intrauterine growth retardation. As a result, the following symptoms are noted:
- Increased heart rate.
- Increase in physical activity, and then its decrease.
- Abdominal volume does not correspond to the duration of pregnancy.
As a rule, such signs appear in the decompensated form of placental insufficiency. If the blood flow disorder has a 1a or 1b degree, identified during a timely examination, then these symptoms do not yet exist, since the hemodynamics are compensated.
Classification

Symptoms depend on the severity of changes in BMD, which are recorded during additional examination. Based on a clinical and gynecological examination, it is impossible to say for sure about this, but one can first judge hemodynamics based on indirect data. Thus, blood flow disorders during pregnancy are classified according to degree:
- 1a degree - changes affect only the uteroplacental part of the blood flow.
- 1b degree - only fetal-placental blood flow is weakened.
- 2nd degree - disturbances affect all hemodynamic processes, but diastolic blood flow is still preserved.
- Grade 3 – a situation where the fetal-placental blood flow has critical disturbances while maintaining or changing the uteroplacental hemodynamics.
This classification is based on the relationship between the speed of uterine and umbilical blood flow. In addition, disorders are identified in individual branches of the afferent artery.
Signs of impaired blood flow from the fetus may not be noticeable to the woman, but the doctor is obliged to pay attention to them.
Consequences
Placental insufficiency poses a risk to fetal development. Therefore, the main obstetric complications concern the condition of the unborn child. The greatest danger comes from severe blood flow disorders, which can have both a chronic and acute course. In this context, degrees 1a and 1b of hemodynamic disorders are not mentioned, as they are the mildest.
Placental abruption
Sudden disturbances in blood flow can be provoked by injuries, thrombosis or embolism of the uterine artery. Then a situation arises when the placenta exfoliates in one of the areas. Depending on its location, the pathology occurs as a central or peripheral type. The following symptoms appear:
- Pain in the area of detachment.
- Local protrusion of the uterine wall.
- Bloody issues.
- Worsening of the fetal condition.
If the detachment is of the central type, then there may be no external discharge at all, but blood seeps into the wall of the uterus, which is why it loses its contractility. This is fraught with atonic bleeding and disseminated blood coagulation (DIC syndrome).
When placental complications are mild, they can be eliminated with adequate therapy.
Miscarriage
In turn, placental abruption causes spontaneous abortion or premature birth, which is included in the concept of miscarriage. This is a situation that obviously all women are afraid of, because losing a child is the worst thing that can happen during this period. Then the following signs appear:
- Pain in the lower abdomen, in the sacrum, rectum.
- Bloody discharge of varying intensity.
- Increased urination.
- Hypertonicity of the uterus.
- Gradual dilatation of the cervix.
If the process is stopped at the threat stage, the child will be saved. But when the placenta has completely detached and an abortion is diagnosed, unfortunately, it is no longer possible to correct anything. In the future, the pathology may be complete or incomplete. When parts of the fetus or membranes are retained in the uterine cavity, there is a risk of infection and severe bleeding, which often ends in hemorrhagic shock or disseminated intravascular coagulation.
Frozen pregnancy

In addition, the fetus may die if left in the uterine cavity. Then a so-called frozen pregnancy is formed. The woman herself can note some symptoms that indicate what happened:
- Fetal movements stop.
- You can't feel his heartbeat.
- The abdomen does not increase in volume.
- Bloody discharge occurs periodically.
- Abdominal pain bothers me.
- Body temperature rises.
- An infection sets in.
A frozen pregnancy must be removed. If this is not done on time, then there is a danger to the life of the woman herself.
Diagnostics

To determine placental blood flow disorders during pregnancy, it is necessary to use additional diagnostic methods. They allow you to determine the type and degree of changes, as well as determine the condition of the fetus. To do this, use the following procedures:
- Blood test for hormones (estrogens, progesterone, human chorionic gonadotropin).
- Ultrasonography.
- Cardiotocogram.
- Doppler.
Some data can also be obtained after a doctor’s examination - the child’s condition can be judged by the heart rate calculated during auscultation. But the most reliable results are obtained after instrumental and laboratory research.
Treatment
In case of disturbance of uteroplacental blood flow of any severity, therapeutic measures are indicated. This is mainly aimed at preventing the progression of the pathology, while normalization of hemodynamics, according to observations, is possible only at stage 1b. At the same time, they try to use all possible means to improve the condition of the fetus. Of course, conservative measures come first. Surgical intervention is used only for complications and for health reasons. In addition, great importance is given to the prevention of placental insufficiency.
Treatment of blood flow disorders during pregnancy is complex - etiotropic, pathogenetic and symptomatic.
Drug therapy

The main means of correcting placental blood flow is the use of medications. When only initial signs of disorders are identified, you can undergo treatment on an outpatient basis. If the deficiency is more pronounced, then hospitalization in a hospital is necessary. This need also exists for extragenital pathology in women. The following drugs are mainly used:
- Antispasmodics (No-shpa, Eufillin).
- Tocolytics (Ginipral, Partusisten).
- Vascular (Actovegin).
- Improving microcirculation (Trental).
- Antiplatelet agents (Curantil).
- Antihypoxants (Instenon).
- Vitamins and microelements (Magne B6, ascorbic acid).
- Metabolic (ATP).
- Hepatoprotectors (Essentiale, Hofitol).
As a rule, it is recommended to undergo two courses of therapy - immediately after diagnosis and at 32-34 weeks. After this, the issue of delivery is decided. This is especially important in severe circulatory disorders. If violations are recorded at stage 1a or 1b, then childbirth occurs naturally.
During pregnancy, only proven medications that have proven their safety and effectiveness are used.
Operation

When placental insufficiency is severe, emergency delivery is necessary. If conservative measures are ineffective, even with mild violations, a decision should be made within 2 days. The most commonly used procedure is a caesarean section. If it is planned before 32 weeks of pregnancy, then it is necessary to proceed from the condition of the fetus and its viability.
When it is necessary to ascertain that a spontaneous abortion has occurred, it is necessary to carry out curettage of the uterine cavity or vacuum extraction of the fetus. In case of a frozen pregnancy, surgical intervention depends on the gestational age and the condition of the woman.
Prevention
To avoid many unpleasant situations during pregnancy, including placental insufficiency, it is necessary to follow preventive recommendations. They mainly relate to lifestyle and include the following principles:
- Healthy eating.
- Rejection of bad habits.
- Walking outdoors.
- Elimination of stress factors.
- Follow all doctor's recommendations.
- Timely treatment of concomitant diseases.
If you take care of your own health during pregnancy, you can prevent disruption of blood flow in the mother-placenta-fetus system. And if this pathology is detected, it is necessary to carry out timely treatment, which will allow saving the child.
During pregnancy, a woman's body undergoes strong hormonal changes. A new circle of blood circulation appears, through which the fetus receives nutrition and oxygen, and also removes waste products. It is the placenta that protects the baby from infections and viruses, and connects two complex circulatory systems: mother and child. A special membrane between these systems prevents the blood in them from mixing with each other. Sometimes, for various reasons, this interaction is disrupted, placental insufficiency occurs, which can lead to negative consequences both for the body of the expectant mother and for the health of the child. That is why it is important to timely analyze the movement of blood in the umbilical cord and uterine arteries of a pregnant woman, check blood circulation in the baby’s vessels and aorta, receive timely treatment and lead a healthy lifestyle. What are the consequences of impaired blood flow during pregnancy, what is its cause and how to avoid it?
Causes of poor blood flow in the uterus
There are several reasons why placental insufficiency occurs. They can both affect the formation of the placenta and appear at later stages of gestation:
- uterine tumors
- genetic defects
- hormonal disorders
- gestosis
- infectious diseases
- structural features
- consequences of abortion
- diabetes
- atherosclerosis
- hypertension
- problems with the adrenal glands and thyroid glands
- multiple births
- Rhesus conflict
Most often, one main risk factor manifests itself. But there may be several reasons at the same time.
Types and degrees of disturbance of uterine blood flow
There are three degrees of impairment:
1st degree
Occurs with the smallest changes in placental blood flow, which are not of a dangerous nature for the child. Within a month, with early detection and proper treatment, there is a high probability of complete recovery without consequences. Divided into two types:
- 1a – failure occurs only in uteroplacental hemodynamics
- 1b – problems arise in the fetoplacental area. The uterine uterus remains complete
2nd degree
In the second degree, both blood flow systems fail. The fetal death rate is about 13%. In a short time, usually up to 10 days, it enters the third stage.
3rd degree
The fetal blood supply is in critical condition. Premature birth is often artificially induced, since the probability of death of an unborn baby is almost 50%.
In the second and third degrees, a caesarean section is most often prescribed. At the first birth, birth occurs naturally, under the careful supervision of a doctor.

Treatment of placental circulatory disorders
Since the main consequence of insufficient blood flow is hypoxia, doctors prescribe drugs that increase the resistance of the fetal tissues and brain to oxygen starvation. In combination, agents that improve heart function and blood microcirculation can be used. If necessary, antiviral and antibacterial drugs are prescribed, as well as agents that prevent the formation of blood clots. The doctor prescribes medications based on the severity of the blood circulation disorder. Sometimes a pregnant woman is offered hospitalization in order to provide her with bed rest, and so that treatment takes place under the close supervision of specialists.


Prevention of pathologies
For timely detection of pathological changes in blood flow between the uterus and the fetus, all future mothers are prescribed Doppler ultrasound three times during pregnancy. It is carried out together with a routine ultrasound and helps to assess the general condition and development of the child, and also gives a complete picture of the state of blood flow in the vessels of the umbilical cord, uterus and fetus. Early detection of disturbances in the functioning of the placenta and blood flow will help to prescribe the drugs necessary for treatment in a timely manner and avoid negative and dangerous consequences for the baby in the future. Doppler sonography is a mandatory test for expectant mothers with bleeding disorders.


It must also be remembered that the health of the baby largely depends on the condition of the mother. Therefore, with food, the body should receive a maximum of macro- and microelements, a sufficient amount of fats, proteins, carbohydrates and liquids. In the absence of swelling, you need to drink at least one and a half liters of water per day. It is necessary to completely eliminate bad habits and try to avoid unnecessary physical and emotional stress. It is important to monitor your weight gain, weigh yourself and measure your abdominal circumference. It is advisable to walk in the fresh air more often and not stay in stuffy rooms for a long time. For pregnant women at risk, prevention is carried out with medication, which helps mother and child interact fully.



Complications such as placental insufficiency or hemodynamic disturbances during pregnancy occur in almost every fourth woman. When blood flow is obstructed, the fetus receives less oxygen and nutrients than is necessary for normal development, which is the main reason for the development of intrauterine fetal hypoxia.
Hemodynamic disturbances during pregnancy in most cases are practically asymptomatic: the expectant mother may not even suspect that the baby is experiencing oxygen starvation. Let's talk about how to suspect a blood flow disorder during pregnancy, why this complication develops, and what to do to normalize it.
The main causes of hemodynamic disturbances during pregnancy.
One of the most important organs during pregnancy is the placenta (baby place), which performs many functions, but primarily ensures the supply of oxygen to the fetus. Oxygen-saturated blood flows from the mother's body to the baby through the placenta, and if this process is disrupted, a lack of oxygen (hypoxia) occurs, followed by intrauterine growth retardation, premature birth and other possible complications, including fetal death.
So, hemodynamic disturbances during pregnancy occur against the background of:
- Extragenital pathology (arterial hypertension, diabetes mellitus, heart defects, thyroid diseases, etc.);
- Late gestosis (preeclampsia);
- Compounded obstetric and gynecological history (uterine fibroids, endometriosis, uterine malformations, abortions, etc.);
- Urogenital infection;
- Moderate to severe anemia;
- Polyhydramnios, multiple pregnancy;
- Bleeding disorders;
- Complicated pregnancy (threat of miscarriage, toxicosis, etc.);
- General exhaustion of the body: with an unbalanced diet, heavy physical labor, weakened immunity, alcoholism, smoking, etc.
How to suspect hemodynamic disturbances during pregnancy?
When uteroplacental blood flow deteriorates, the woman does not notice any special changes in her general well-being. This leads to the fact that a mild degree of circulatory disturbance in the placenta progresses, along with which the condition of the fetus worsens.
Hemodynamic disturbances during pregnancy can be suspected based on the following signs:
Changes in the frequency of fetal movements (too vigorous or, conversely, weak movement).
Starting from the 28th week of pregnancy, all women are recommended to carry out the so-called “10 movements test”. Normally, within 12 hours, the baby should make itself felt at least 10 times, while both a single push and their simultaneous sequence are considered to be moving.
Inconsistency between the size of the abdomen and the gestational age.
If blood flow is disrupted during pregnancy, the baby does not receive enough oxygen and nutrients, as a result of which it lags behind in physical development. Therefore, when visiting a antenatal clinic, the expectant mother has her abdominal circumference measured and the height of the uterine fundus determined in order to assess the dynamics.
The appearance of bloody discharge from the genital tract.
This sign indicates a terminal condition of the fetus - premature placental abruption, in which immediate emergency care must be provided. To do this, an emergency ultrasound examination of the uterus is performed, assessing the condition of the fetus, and a decision is made on emergency surgery, if the gestational age allows, or on prolongation of pregnancy.
How to identify hemodynamic disturbances during pregnancy? Doppler.
Doppler is one of the types of ultrasound examination, in which the attention of the diagnostician is focused on the state of blood flow in the uterine and umbilical arteries, placenta, brain and aorta of the fetus. The research method is based on the Doppler effect - a change in sound vibrations depending on the speed of blood flow.
Doppler measurements distinguish the following degrees of blood flow disturbance:
- 1A degree: blood flow is impaired in the arteries of the uterus
- Grade 1B: blood flow is impaired in the umbilical cord arteries
If left untreated, it progresses to stage 2 after about 3 weeks.
Tactics: hospital treatment, Doppler monitoring and CTG (cardiotocography) of the fetus every 5-7 days, if the condition worsens - daily.
2nd degree: disturbance of blood flow in the arteries of the uterus and umbilical cord.
If left untreated, it progresses to grade 3 in about 1-1.5 weeks.
Tactics: treatment in a hospital, Dopplerography and CTG of the fetus every 2 days, if the child’s condition worsens and the pregnancy is more than 32 weeks - emergency surgical delivery.
3rd degree: critical disturbance of the blood flow of the umbilical cord vessels with normal or impaired blood flow in the uterine arteries.
Tactics: emergency delivery.
Doppler testing is indicated for all women, starting from 16-18 weeks - with a complicated course, and at 20-22 weeks - with a normal pregnancy.
Don't self-medicate! If you suspect a deterioration in uteroplacental blood flow, immediately seek help from a doctor, because the count may not be days, but hours. Have an easy pregnancy and childbirth!



